
Options for Breech Presentation
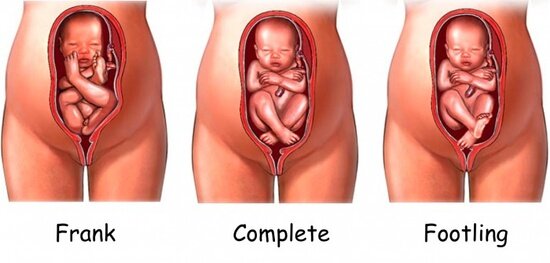
A baby that is breech is positioned in such a way that the baby's bottom or feet will be delivered first, rather than the more common head-down position. Delivery via cesarean section is the most common recommendation for babies that do not turn head-down before labor starts.
Recently, the American College of Obstetrics and Gynecology has released the statement the the breech delivery of a singleton may be reasonable, and does not always require that the baby be born via cesarean!
Read the full article below...
ACOG ISSUES GUIDANCE ON EXTERNAL CEPHALIC VERSION
All eligible women with breech presentations who are near term should be offered external cephalic version (ECV) to cut down on the number of cesarean deliveries, according to a new practice bulletin from the American College of Obstetricians and Gynecologists (ACOG).
ECV involves applying pressure to a woman's abdomen to turn the fetus from breech to vertex presentation, which increases the likelihood of a vaginal delivery.
The February bulletin, developed by ACOG's Committee on Practice Bulletins—Obstetrics and published in the February issue of Obstetrics & Gynecology, summarizes the latest evidence surrounding ECV and recommendations for its use, updating recommendations from February 2000.
"[ECV] is a valuable management technique and, in a properly selected population, poses little risk to either the woman or the fetus. If successful, ECV provides a clear benefit to the woman by allowing her an opportunity for a successful vertex vaginal delivery," the committee writes.
Interest in the technique has increased in light of medicine's movement to decrease cesarean deliveries, which are often thought to be the only appropriate option for breech presentations. Previous studies have shown there are fewer cesarean deliveries among women who have undergone successful ECV compared with those for whom the procedure was not attempted, the committee reports.
Six Points in Summary
ACOG's level A recommendation (based on good and consistent evidence) says, "all women who are near term with breech presentations should be offered an ECV attempt if there are no contraindications."
Level B findings (based on limited and inconsistent evidence) include three points:
Fetal presentation should be documented beginning at 36 weeks of gestation to allow for ECV. If spontaneous version is going to happen, it will likely have happened by then. Likewise, by that time, risk for a spontaneous reversion after ECV is lower than earlier in gestation.
Having had a previous cesarean delivery is not linked with lower rate of success; however, whether it magnifies risk for uterine rupture is not known.
Evidence supports using parenteral beta-agonist tocolysis to improve ECV success.
Two recommendations are based primarily on consensus and expert opinion:
Physicians should study fetal well-being and contraction patterns with a nonstress test or biophysical profile before and after ECV.
The procedure should be attempted only in settings where the option of a cesarean is readily available.
If, after ECV, the breech persists, the best mode of delivery should depend on expertise of the healthcare provider.
"Thus, a planned term singleton breech vaginal delivery may be reasonable in some cases with full patient counseling and consent," the bulletin says.
Obstet Gynecol. 2016;127:412-413.